
Long COVID patients among those likely to be targeted under new Medicaid work requirements
Long COVID patients already struggle to access SSI. Now, Trump's Medicaid work requirements could see chronically ill and disabled people without documentation lose coverage

Last week, Donald Trump signed his so-called Big Beautiful Bill, officially condemning millions of the most vulnerable Americans to lose their health insurance, handing an eye-popping budget to ICE, and of course, providing another tax break to the ultra-wealthy.
Among the cruel cuts? A provision stating that Medicaid recipients must work, volunteer, or attend education or training for a minimum of 80 hours each month. Defenders of the bill point out that this work requirement contains exemptions for the elderly, pregnant, caregivers, and yes, the disabled. But disabled according to whose definition?
That’s right, disabled as defined by the very same government snatching back benefits in the first place. The exemptions in the bill are based on the strict SSI definition of disability, and, while the law will be administered at the state level, documentation will doubtless come in play. The bill does not allow for states to include additional exemptions of their own. Significant questions remain concerning enforcement, but the goal of the requirement is clear: reduce spending by booting people off Medicaid.
According to the State Health Access and Data Assistance Center (SHADAC), only 10.1% of Medicaid recipients qualified for Medicaid through a disability pathway in 2023, but 33.9% of recipients self-identify as disabled. There are many reasons for this discrepancy. SSI and SSDI are notoriously difficult and time-consuming to qualify for, with some people waiting years to receive benefits, and others never receiving them at all.
Wait times have soared in recent years, with initial decisions taking an average of 220 days - or 7.5 months. In 2022, only about 1/3 of initial disability applications were approved, with rejected applicants then having file an appeal within the next 60 days. From there, you’ll wait another 7 months for your reconsideration decision. If rejected again, you’ll be waiting an average of 15 months to get a hearing before an SSA law judge.
Overall, about two-thirds of disabled Medicaid enrollees do not receive SSI, meaning they haven’t gone through the often-lengthy process of documenting their disability with the state. And SSI enrollment is lowest among younger folks, as seen in this 2023 data from KFF:
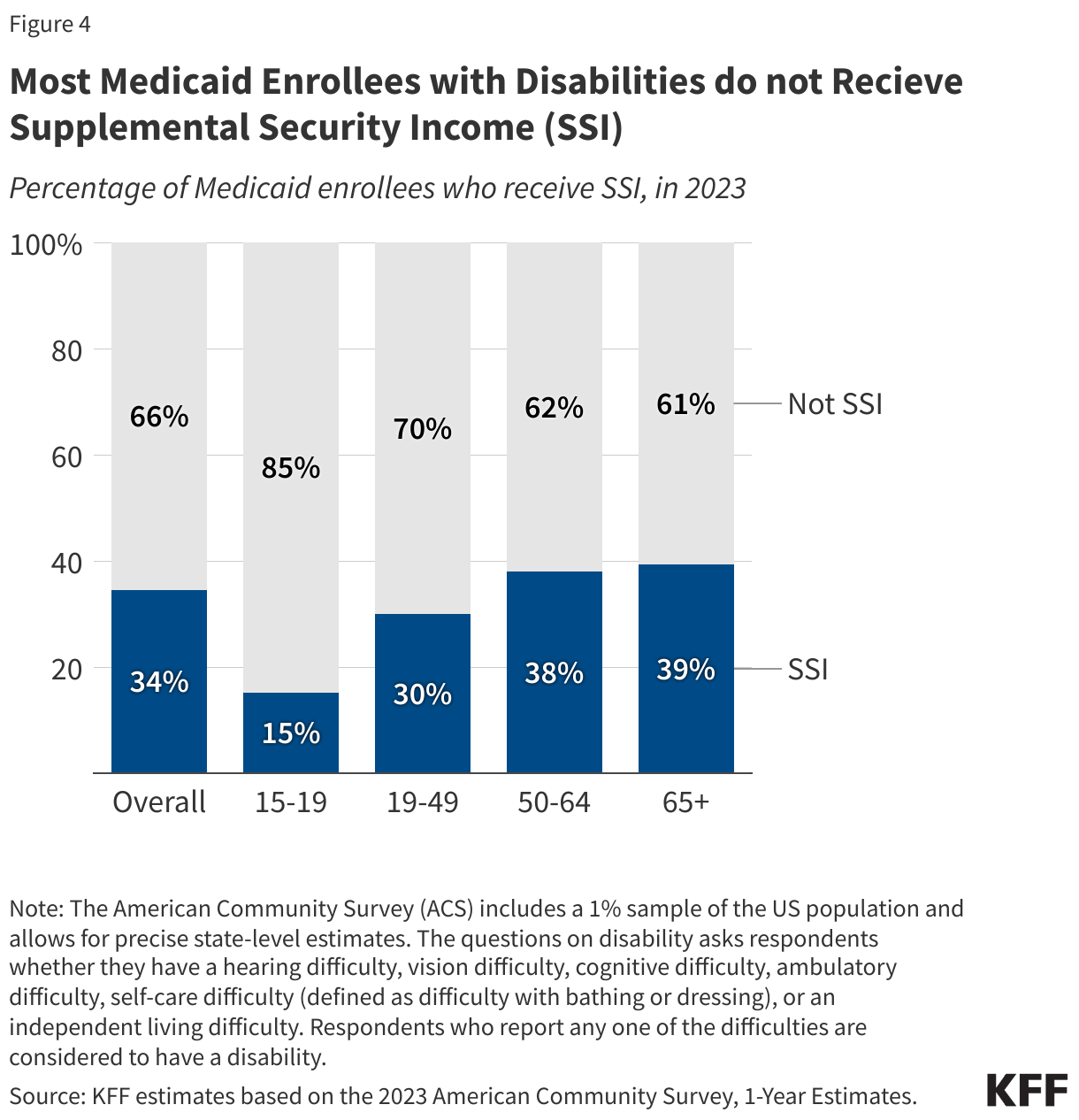
Among 19-49 year olds, people in the prime of life, 70% of disabled people on Medicaid do not have SSI. This age group is ripe for targeting with work requirements, falling as they do within peak working years, yet failing to have the medical paperwork on file they may need for an exemption. It’s likely that documentation will be a hurdle for anyone who doesn’t currently have it. According to SHADAC:
during New Hampshire’s 2019 implementation of its Medicaid work requirement, the Granite Advantage Health Care Program, the state received only 1,951 exemption requests based on medical frailty—far fewer than expected given that more than 10,700 individuals had previously self-attested to that status. This gap highlights the significant administrative barriers that may prevent eligible individuals with self-reported disabilities from securing exemptions under Medicaid work requirements.
In other words, when means testing or onerous bureaucracy is introduced, the number of people accessing a public benefit plummets. This, critics are quick to point out, is more often than not the point of means testing and bureaucracy; to reduce the burden on the state. Far from weeding out “fraud” or “graft,” it simply weeds out the most vulnerable.
But beyond universal bureaucratic hurdles, patients suffering from illnesses that are less well-understood, particularly those without objective biomarkers and which appear invisible, will face additional challenges. Many types of Long COVID, an umbrella diagnosis that is both new and stigmatized, fall squarely in this category.
Reporting has tracked the difficulties Long COVID patients have had accessing SSI for years. In 2022, Betsy Ladyshetz, now co-founder of The Sick Times, wrote about the issue for KFF Health News, noting that, “July 2021 guidance recognized long covid under the Americans with Disabilities Act but didn’t extend to the Social Security Administration, which runs benefit programs.” A year later, in 2023, reporter Morgan Stephens of CNN again covered the story, but no progress had been made. “Nearly three years into the pandemic, long Covid still isn’t included on SSA’s listing of qualifying disabilities,” Morgan reported.
Charlie McCone, a 35-year-old in the Bay Area, first applied for SSDI in 2022 after a COVID reinfection left him bedbound and unable to work. Today, he is unable to walk around the block without suffering debilitating migraines and fatigue. He can work a maximum of about two hours on a good day. Despite legal assistance, he was immediately denied for SSDI during his initial application, and is now on his 3rd stage of appeal awaiting a court hearing. Of his experience with SSA, he says:
It has been the most demoralizing, undignified, and enraging experience imaginable. The process is already egregious for people with the most explicit and measurable disabilities, my attorney says she regularly gets denials for clients with stage 4 terminal cancer, and hence the process is nearly impossible for those with invisible disabilities harder to measure within the framework of conventional medicine and safety net, like Long COVID. The idea SSA can easily determine who is disabled and not is a catastrophic misunderstanding. People with severe ME/CFS and Long COVID are experiences some of the most disabling conditions known to the history of man. These are people unable to leave their bed or house, and unable sit at a desk or concentrate for longer than an hour a day (sometimes minutes) — and almost always are subjected to years or denial, appeal, just for the chance to live in abject poverty (avg SSDI payout is $1,538).
The difficulty Long COVID patients have had accessing SSI and SSDI was the subject of a letter written by the Senate HELP Committee to then-Social Security Administration (SSA) Commissioner Martin O’Malley in August 2024. Sent by Senator Tim Kaine and signed by fellow members Sens. Tammy Duckworth, Ed Markey, Angus King Jr., Bernie Sanders, Tina Smith, and Richard Blumenthal, the letter pertains to the barriers people with Long COVID are encountering as they try to access Social Security benefits.
This letter made several requests of SSA, including that SSA begin tracking and publishing data on applications relating to Long COVID, that SSA review the NASEM report and create a new Long COVID ruling with input from patient groups, and that SSA restore the “treating physician rule”
The “treating physician rule” was a rule that, prior to 2017, an applicant's primary care physician or main treating physician would be weighted more heavily over the opinions of physician(s) who met with the applicant briefly in the course of SSA proceedings. As for the other requests, they point to both a concerted effort to bury Long COVID (ongoing refusal to release data related to Long COVID applications and rejections at SSA) as well as an utter failure to modernize and accommodate the existence of Long COVID at all (urging SSA to review the NASEM report and introduce new guidance to evaluate Long COVID patients).
All of these issues are likely to remain relevant as Medicaid purges the “able bodied” who do not complete requisite work hours from its rolls. SSA is charged with determining who is disabled, yet, as a body, it is unfamiliar with the definition of Long COVID, has yet to standardize guidance concerning Long COVID, fails to prioritize the testimony of treating physicians for Long COVID patients, and fails to provide statistics about the rejection rate of Long COVID applicants.
Since 2020, the pandemic has been disabling working-age people at unprecedented rates. Some sufferers know they have Long COVID and identify themselves as such; others don’t, due to deliberately poor public health communication or to stigma. There are Long COVID patients who are too sick to work, who do not have any real treatment options, who also may not have language to describe their illness. Many of these people, importantly, may not have laboratory testing confirming their illness due to the nascent and ongoing nature of Long COVID research.
In order to receive SSI/SSDI, applicants must demonstrate to the Social Security Administration that they have a medical condition that is “expected to last at least one year”. Here again, Long COVID minimization and stigmatization may hinder patients as they attempt to access work requirement waivers. Reporting has repeatedly highlighted optimistic studies wherein patients recovered within months, and these reports could be used to argue that Long COVID patients can’t be certain that their illness will last beyond a year.
All this is to say that attaching work requirements to Medicaid will accomplish something, but that something won’t be increasing the labor pool. Work requirements won’t get people who are too disabled to work, working. They will save the state money by snatching healthcare away from very sick people who are suffering, but don’t have the documentation to prove it- in some cases, simply because the infrastructure to document their illness barely exists. Such requirements will prosecute people who’ve been disabled by a virus that is being categorically denied and disappeared by the state, as its victims are labeled lazy liars.
On the flip side of the states’ targeting of disabled populations is its targeting of immigrants. As violent raids across the country continue to snatch mothers, fathers, neighbors and friends from their communities, the economic impact of these amped up detentions and deportations have begun to be noted even by critics on the right. Speaking this week, Agriculture Secretary Brooke Rollins said of farm laborers:
There will be no amnesty. The mass deportations continue, but in a strategic way. And we move the workforce toward automation and 100% American participation, which with 34 million able-bodied on Medicaid we should be able to do fairly quickly.
It’s a stunning and stark example of the intersectional nature of oppressions. As the state arrests and deports one marginalized group- undocumented migrant workers - it now expects to call on another - poor, mostly disabled people on Medicaid- to step in and take over that labor, so the upper classes don’t experience any disruption to their expected services.
People with Long COVID, of course, are not the first nor only chronically ill and disabled people who will be affected by these cuts. There are plenty of conditions that have been viewed as “malingering” and cast as “hysteria” prior to 2020, including other post-viral illnesses which, due to lack of funding, continue to be difficult to diagnose and treat. But since the number of patients “living off of” the state continues to increase at an unprecedented rate, the hatred directed at these populations ramps up accordingly.
The US isn’t the only place we’re watching these ideas gain support. In the UK, harsh bills attempting to force disabled people into work have been pushed forward by, not the conservatives, but the Labour Party. In March, the UK government released its “Pathways to Work: Reforming Benefits and Support to Get Britain Working Green Paper” aimed at cutting billions from its disability programs. Just as in the US, government officials claim that they are going to sort out who is “really” disabled and who is “faking”, who is “lazy”; therefore, the legislated push to force disabled people into work is righteous, not cruel.
To review: state fails to control virus. State negligently allows people to become infected. State claims no one can be hurt by this virus. When people subsequently report being hurt by virus, state calls them liars. When people try to collect benefits, state denies them, then begins cutting them. When people try to access healthcare, state tells them to get back to work and runs propaganda campaign to paint them as lazy and dishonest.
I’d be remiss if I didn’t mention that this framing- that people with Long COVID are lazy, that they are fakers, that they are crazy, and that they need to get back to work- has a clear place within the COVID normalization project and makes perfect sense when viewed as part of that larger political whole.
I’d be remiss, too, if I didn’t mention that this is why it is so very disturbing to see people on all parts of the political spectrum repeat this heavily politicized outlook about Long COVID, a disease which can afflict anyone after any infection. People with Long COVID are not liars, fakers, crazy, paranoid, or lazy. They were simply hurt by a circulating virus that can disable human beings, that has killed tens of millions over the last five years.
When you mock and stigmatize Long COVID patients for sharing their stories, advocating for COVID mitigations, and describing their symptoms, you are doing propaganda work for the state. You are advancing the state’s interests; in this case, throwing disabled people who are too ill to work off of Medicaid by fostering doubt about the legitimacy of their disease.
There is no scientific doubt about the existence or legitimacy of Long COVID, only political doubt. But it is this political doubt - and the lack of a political framework to acknowledge and support people with the disease- that will enable the government to deny patients benefits, subject them to impossible work requirements, and snatch away the health insurance they need to survive.
Sadly, the only recognized test by SSDI to prove myalgic encephalomyelitis caused by long covid is a 2 day cardiopulmonary exercise test. It is $3000 out of pocket and causes serious post exertional malaise (PEM). Mine lasted 4 weeks after the test. Only people who can afford it, have access to it (limited places offer it), and are willing to damage their body will get the documentation they need to prove their condition. It’s another injustice for us.
The doctor contracted by the SSA to examine me for my long COVID-related SSDI case spent a total of three minutes with me, no exaggeration. When my husband wheeled me into the room in my mobility chair, the doctor turned, looked at me, and said, “you’re a little young to be in that thing, aren’t you?” It was, start to finish, the most humiliating medical experience of my then 48 years of life.